Care for persons exposed to sexual violence: psychological treatment of complex PTSD – A Systematic Review including Ethical Aspects
 Share on Facebook
Share on Facebook
 Share on LinkedIn
Share on LinkedIn
 Share via Email
Share via Email
Conclusions
- There are too few well-conducted studies to be able to draw any conclusions about the effects of psychological treatments for persons with complex post-traumatic stress disorder (PTSD).
- People with complex PTSD may feel fear or shame when talking about their experiences of sexual violence. They may also be afraid of relatives who are their perpetrators or worry about dissemination of private information. Being exposed to sexual violence is an extremely serious assault involving violations of the person's integrity, self-determination, and dignity. It can bring a significant negative impact on health, and harm the person's opportunities to live a safe, rich, and independent life. This means that values such as health and well-being, autonomy, and integrity as well as professional and research ethical aspects are important to consider when caring for people with complex PTSD.
Background
The diagnose complex post-traumatic stress disorder (PTSD) has recently been coined to describe problems related to psychological trauma that is overlapping and yet different to PTSD. The diagnosis describes a traumatization that involves problems included in the PTSD diagnosis, in addition to problems with self-image, social relationships and emotion regulation. The diagnose is particularly common after traumas such as sexual violence. PTSD is a form of psychological trauma. PTSD is a psychiatric diagnosis that describes a condition where a person suffers problems that arose or worsened in connection with a traumatic event. The symptoms include re-experiences of a traumatic event during flashbacks and nightmares, and feeling of tension, vigilance, and avoidance of things reminiscent of the event. Violence in a close relationship is estimated to be related to nearly half of the total burden of PTSD.
To meet the diagnostic criteria for complex PTSD, the person must meet the criteria of ICD-11 for both PTSD and "disturbances in self-organization" (DSO). DSO includes three areas: disturbances in emotion regulation, consistently negative self-image and great difficulty maintaining relationships. These symptoms should be persistent and pervasive, which means that they affect the individual's life in almost all situations in everyday living, over a long period of time.
An excessive focus on what kind of event that caused the symptoms risks forming an image that treatments must be adapted to a specific trauma. Therefore, this report does not consider the reason behind complex PTSD.
As there are uncertainties in how people with complex PTSD should be handled in care, this report investigates the body of evidence for psychological treatment methods for patients with complex PTSD.
Aim
The aim of this report is to evaluate the body of evidence for psychological treatment methods for patients with complex PTSD.
Method
This systematic review has been conducted in accordance with the PRISMA statement. The protocol is registered in Prospero https://www.crd.york.ac.uk/prospero/CRD 42024519015.
For a study to be included in this systematic review, the following inclusion criteria needs to be fulfilled.
Inclusion criteria:
Population
Persons 18 years of age or older diagnosed with complex PTSD according to ICD-11, or adults with diagnosed PTSD and symptoms indicative of complex PTSD (disturbances in self-organization including affect dysregulation, negative self-concept, and disturbances in relationships).
Intervention
Psychological treatments including talking therapies based on a psychological theory provided by health care in Sweden. Descriptions of various assessments before treatment are not included.
Control
A different treatment than that given to the intervention group. The treatment must be relevant to a Swedish context and can be treatment as usual, medication, waiting list or active control treatment.
Outcome
Symptoms of complex PTSD, degree of remission and level of functioning. Symptoms of complex PTSD refers to both symptoms of PTSD and DSO, based on how the diagnosis is defined in ICD-11.
Study design
Randomized controlled trials (RCTs) and systematic reviews based on RCTs.
Language: English, Swedish, Danish, and Norwegian.
Search date: The final literature search was conducted in April 2023.
Databases searched:
- CINAHL (EBSCO)
- Cochrane Library (Wiley)
- Criminal Justice Abstracts (EBSCO)
- EMBASE (Embase.com)
- Ovid MEDLINE(R) ALL
- APA Psycinfo (EBSCO)
- PTSDpubs (ProQuest)
- Scopus (Elsevier)
- Social Services Abstracts (ProQuest)
- Sociological Abstracts (ProQuest)
- SocINDEX (EBSCO)
Supplementary searches for ongoing and published systematics reviews and HTA reports were made in the following databases:
- The Campbell Collaboration
- Epistemonikos
- International HTA Database
- PROSPERO
In addition, searches for ongoing clinical trials were conducted in ClinicalTrials.gov and the International Clinical Trials Registry Platform.
Client/patient involvement: No
Results
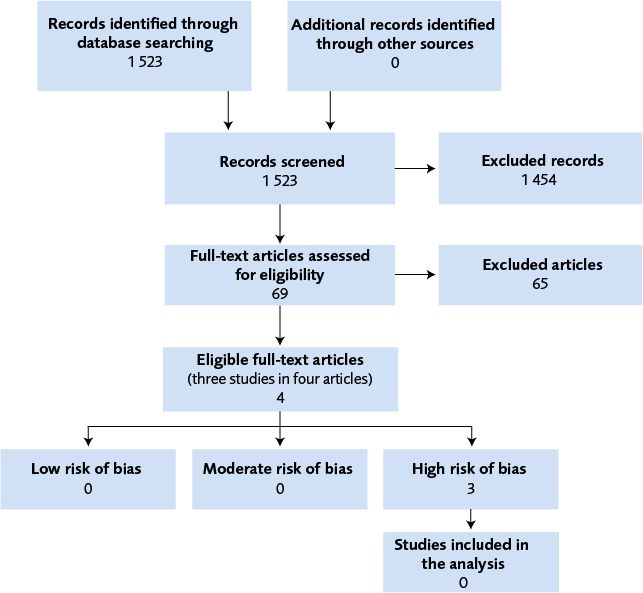
This systematic review identified three randomized controlled studies that have investigated psychological treatment methods for persons with complex PTSD or with PTSD and symptoms of complex PTSD. However, none of the studies holds low or moderate risk of bias. The risk of bias was assessed to be high in all three studies due to high attrition rate, deficiencies in outcome measurements, as well as reporting bias.
The three studies, conducted in the Netherlands or in Lithuania, were published between 2006 and 2021. The evaluated interventions were:
- mindfulness-based intervention compares to waiting list
- phase-based treatment compared to immediate trauma-focused treatment
- stabilizing group treatment based on psychoeducation and cognitive behavioural therapy compared to treatment as usual.
The studies that were found to be irrelevant, was excluded because they did not study people with complex PTSD and did not report outcomes that cover the three DSO symptom groups.
Ethics
Not caring for or treating a person exposed to sexual violence can cause a high risk of negative consequences for the patient. Risk assessment, diagnosis, care, and support is therefore very important for the person's future health and quality of life. Although there is a lack of scientific support for interventions in complex PTSD, there are risks in not caring and treating when there is scientific support for the treatment of PTSD, depression and other psychiatric conditions that are common in people who have been sexually abused.
Relevant justice and equality aspects primarily concern accessibility. There are various barriers that can stand in the way for people with complex PTSD, hindering them to seek care. They may sense fear or anxiety to talk about experiences of sexual violence that may be associated with stigma. There may also be fear of blame from relatives who are possibly perpetrators or fear of private information being spread. In addition, it can be difficult for healthcare professionals to identify people in the target group whom they might get in touch with when they seek help for other problems.
It is important that the consent process for participation in research is adapted to needs that may exist in this group. A further aspect of informed consent concerns voluntariness in relation to healthcare professionals. There may be a risk that you want to be accommodating and find it difficult to say no if the question is raised by healthcare staff.
Discussion
SBU found no RCTs with low or moderate risk of bias that examined whether psychological treatments are effective in alleviating symptoms of complex PTSD in people diagnosed with complex PTSD or undiagnosed, but with clear symptoms of complex PTSD. Three relevant RCTs with adult participants were identified, but all of them were judged to have a high risk of bias. Regarding research on complex PTSD, there are several important ethical aspects to consider.
The diagnosis of complex PTSD was formally accepted six years ago with the completion of the International Classification of Diseases ICD-11 by the WHO in 2019. However, the disorder has been discussed for much longer than that. Symptoms of PTSD can be successfully treated across a wide range of PTSD patient populations, with several different psychological treatments, including a variety of cognitive and behavioural therapy treatment protocols. But the state of knowledge is still unclear regarding DSO symptoms.
Conflicts of Interest
In accordance with SBU’s requirements, the experts and scientific reviewers participating in this project have submitted statements about conflicts of interest. These documents are available at SBU’s secretariat. SBU has determined that the conditions described in the submissions are compatible with SBU’s requirements for objectivity and impartiality.
Project group
Experts
- Filip Arnberg, Uppsala University, Uppsala, Sweden
- Ulrik Kihlbom, Karolinska institutet, Stockholm, Sweden
SBU
- Gunilla Fahlström, project manager
External reviewers
Sean Perrin, Lund University, Lund
Flow chart
Appendices
- Search strategies (PDF)
- Excluded articles (PDF)
- Studies with high risk of bias (PDF)
Reference list
- Regeringen. 2023:Regeringsbeslut 2023-03-09, S2023/00970 (delvis) Uppdrag att genomföra insatser för att stödja en jämlik och kunskapsbaserad hälso- och sjukvård för personer som har utsatts för sexuellt våld. Stockholm: Socialdepartementet. [accessed May 6 2024]. Available from: https://www.regeringen.se/contentassets/58554cc9664545478e1221630456ab30/uppdrag-att-genomfora-insatser-for-att-stodja-en-jamlik-och-kunskapsbaserad-halso--och-sjukvard-for-personer-som-har-utsatts-for-sexuellt-vald.pdf.
- WHO. World report on violence and health. Geneva, Switzerland: World Health Organization, (WHO); 2002. [accessed May 7 2024]. Available from: https://www.who.int/publications/i/item/9241545615.
- NCK. Våld och hälsa: En befolkningsundersökning om kvinnors och mäns våldsutsatthet samt kopplingen till hälsa. NCK-rapport 2014:1. Uppsala; 2014. [accessed May 3 2024]. Available from: https://kunskapsbanken.nck.uu.se/nckkb/nck/publik/fil/visa/418/NCK-rapport_prevalens_Vald_och_halsa_www.pdf.
- Kessler RC, Aguilar-Gaxiola S, Alonso J, Benjet C, Bromet EJ, Cardoso G, et al. Trauma and PTSD in the WHO World Mental Health Surveys. Eur J Psychotraumatol. 2017;8(sup5):1353383. Available from: https://doi.org/10.1080/20008198.2017.1353383.
- SBU. Psykologisk, psykosocial och annan icke-farmakologisk behandling av posttraumatiskt stressyndrom (PTSD) hos vuxna. Stockholm: Statens beredning för medicinsk och social utvärdering (SBU); 2019. SBU Kommenterar 2019_12. [accessed May 3 2024]. Available from: https://www.sbu.se/2019_12.
- International Classification of Diseases, Eleventh Revision (ICD-11). World Health Organization, WHO; 2019/2021. [accessed March 31 2025]. Available from: https://icd.who.int/browse11.
- Frans O, Rimmö PA, Aberg L, Fredrikson M. Trauma exposure and post-traumatic stress disorder in the general population. Acta Psychiatr Scand. 2005;111(4):291-9. Available from: https://doi.org/10.1111/j.1600-0447.2004.00463.x.
- Cloitre M, Miranda R, Stovall-McClough KC, Han H. Beyond PTSD: Emotion regulation and interpersonal problems as predictors of functional impairment in survivors of childhood abuse. Behavior Therapy. 2005;36(2):119-24. Available from: https://doi.org/https://doi.org/10.1016/S0005-7894(05)80060-7.
- Maercker A, Brewin CR, Bryant RA, Cloitre M, van Ommeren M, Jones LM, et al. Diagnosis and classification of disorders specifically associated with stress: proposals for ICD-11. World Psychiatry. 2013;12(3):198-206. Available from: https://doi.org/10.1002/wps.20057.
- Maercker A, Hecker T, Augsburger M, Kliem S. ICD-11 Prevalence Rates of Posttraumatic Stress Disorder and Complex Posttraumatic Stress Disorder in a German Nationwide Sample. J Nerv Ment Dis. 2018;206(4):270-6. Available from: https://doi.org/10.1097/nmd.0000000000000790.
- Wolf EJ, Miller MW, Kilpatrick D, Resnick HS, Badour CL, Marx BP, et al. ICD-11 Complex PTSD in US National and Veteran Samples: Prevalence and Structural Associations with PTSD. Clin Psychol Sci. 2015;3(2):215-29. Available from: https://doi.org/10.1177/2167702614545480.
- Bondjers K, Hyland P, Roberts NP, Bisson JI, Willebrand M, Arnberg FK. Validation of a clinician-administered diagnostic measure of ICD-11 PTSD and Complex PTSD: the International Trauma Interview in a Swedish sample. Eur J Psychotraumatol. 2019;10(1):1665617. Available from: https://doi.org/10.1080/20008198.2019.1665617.
- Herman JL. Trauma and recovery. New York: Basic Books; 1992.
- van der Kolk BA, Roth S, Pelcovitz D, Sunday S, Spinazzola J. Disorders of extreme stress: The empirical foundation of a complex adaptation to trauma. J Trauma Stress. 2005;18(5):389-99. Available from: https://doi.org/10.1002/jts.20047.
- Bryant RA. The complexity of complex PTSD. Am J Psychiatry. 2010;167(8):879-81. Available from: https://doi.org/10.1176/appi.ajp.2010.10040606.
- Friedman MJ, Resick PA, Bryant RA, Brewin CR. Considering PTSD for DSM-5. Depress Anxiety. 2011;28(9):750-69. Available from: https://doi.org/10.1002/da.20767.
- Socialstyrelsen. Nationella riktlinjer för vård vid depression och ångestsyndrom: Stöd för styrning och ledning. Stockholm: Socialstyrelsen; 2021. Nationella riktlinjer. [accessed May 3 2024]. Available from: https://www.socialstyrelsen.se/kunskapsstod-och-regler/regler-och-riktlinjer/nationella-riktlinjer/riktlinjer-och-utvarderingar/depression-och-angest/.
- Forbes D. Effective treatments for PTSD : practice guidelines from the international society for traumatic stress studies. 3 ed. New York: The Guilford Press; 2020.
- Wright SL, Karyotaki E, Cuijpers P, Bisson J, Papola D, Witteveen A, et al. EMDR v. other psychological therapies for PTSD: a systematic review and individual participant data meta-analysis. Psychol Med. 2024:1-9. Available from: https://doi.org/10.1017/s0033291723003446.
- SBU. Internetförmedlad psykologisk behandling: jämförelse med andra behandlingar vid psykiatriska syndrom. Stockholm: Statens beredning för medicinsk och social utvärdering (SBU); 2021. SBU Utvärderar 337. [accessed May 3 2024]. Available from: https://www.sbu.se/337.
- McLean CP, Levy HC, Miller ML, Tolin DF. Exposure therapy for PTSD: A meta-analysis. Clin Psychol Rev. 2022;91:102115. Available from: https://doi.org/10.1016/j.cpr.2021.102115.
- Asmundson GJG, Thorisdottir AS, Roden-Foreman JW, Baird SO, Witcraft SM, Stein AT, et al. A meta-analytic review of cognitive processing therapy for adults with posttraumatic stress disorder. Cogn Behav Ther. 2019;48(1):1-14. Available from: https://doi.org/10.1080/16506073.2018.1522371.
- Cloitre M, Courtois CA, Charuvastra A, Carapezza R, Stolbach BC, Green BL. Treatment of complex PTSD: results of the ISTSS expert clinician survey on best practices. J Trauma Stress. 2011;24(6):615-27. Available from: https://doi.org/10.1002/jts.20697.
- Darby RJ, Taylor EP, Cadavid MS. Phase-based psychological interventions for complex post-traumatic stress disorder: A systematic review. Journal of Affective Disorders Reports. 2023;14:100628. Available from: https://doi.org/https://doi.org/10.1016/j.jadr.2023.100628.
- Coventry PA, Meader N, Melton H, Temple M, Dale H, Wright K, et al. Psychological and pharmacological interventions for posttraumatic stress disorder and comorbid mental health problems following complex traumatic events: Systematic review and component network meta-analysis. PLoS Med. 2020;17(8):e1003262. Available from: https://doi.org/10.1371/journal.pmed.1003262.
- Finch J, Ford C, Grainger L, Meiser-Stedman R. A systematic review of the clinician related barriers and facilitators to the use of evidence-informed interventions for post traumatic stress. J Affect Disord. 2020;263:175-86. Available from: https://doi.org/10.1016/j.jad.2019.11.143.
- Smith JR, Workneh A, Yaya S. Barriers and Facilitators to Help-Seeking for Individuals With Posttraumatic Stress Disorder: A Systematic Review. J Trauma Stress. 2020;33(2):137-50. Available from: https://doi.org/10.1002/jts.22456.
- Bäärnhielm S, Ramel B, Theunis E, Mijaljica G, Dyster-Aas J, Arnberg FK. Posttraumatiskt stressyndrom (PTSD) och komplex PTSD (CPTSD): En klinisk kunskapsuppdatering. Läkartidningen. 2024;121:23090.
- Bramer WM, Giustini D, de Jonge GB, Holland L, Bekhuis T. De-duplication of database search results for systematic reviews in EndNote. J Med Libr Assoc. 2016;104(3):240-3. Available from: https://doi.org/10.3163/1536-5050.104.3.014.
- The EndNote Team. EndNote. Philadelphia, PA: Clarivate; 2013.
- Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan — a web and mobile app for systematic reviews. Systematic Reviews. 2016;5(210).
- Covidence systematic review software. Melbourne, Australia: Veritas Health Innovation; 2023 Available from: https://www.covidence.org/. Available from: https://www.covidence.org/.
- SBU. Utvärdering av insatser i hälso- och sjukvården och socialtjänsten: En metodbok. Stockholm: Statens beredning för medicinsk och social utvärdering (SBU); 2023. [accessed May 6 2024]. Available from: https://www.sbu.se/metodbok.
- SBU. Etiska aspekter på insatser inom hälso- och sjukvården. En vägledning för att identifiera relevanta etiska aspekter. Stockholm: Statens beredning för medicinsk och social utvärdering, (SBU); 2021. [accessed May 6 2024]. Available from: https://www.sbu.se/globalassets/ebm/etiska_aspekter_halso_sjukvarden.pdf.
- Karatzias T, Murphy P, Cloitre M, Bisson J, Roberts N, Shevlin M, et al. Psychological interventions for ICD-11 complex PTSD symptoms: systematic review and meta-analysis. Psychol Med. 2019;49(11):1761-75. Available from: https://doi.org/10.1017/s0033291719000436.
- Dumarkaite A, Truskauskaite-Kuneviciene I, Andersson G, Kazlauskas E. The Effects of Online Mindfulness-Based Intervention on Posttraumatic Stress Disorder and Complex Posttraumatic Stress Disorder Symptoms: A Randomized Controlled Trial With 3-Month Follow-Up. Front Psychiatry. 2022;13:799259. Available from: https://doi.org/10.3389/fpsyt.2022.799259.
- Dumarkaite A, Truskauskaite-Kuneviciene I, Andersson G, Mingaudaite J, Kazlauskas E. Effects of Mindfulness-Based Internet Intervention on ICD-11 Posttraumatic Stress Disorder and Complex Posttraumatic Stress Disorder Symptoms: a Pilot Randomized Controlled Trial. Mindfulness (N Y). 2021;12(11):2754-66. Available from: https://doi.org/10.1007/s12671-021-01739-w.
- Dorrepaal E, Thomaes K, Smit JH, van Balkom AJ, Veltman DJ, Hoogendoorn AW, Draijer N. Stabilizing group treatment for complex posttraumatic stress disorder related to child abuse based on psychoeducation and cognitive behavioural therapy: a multisite randomized controlled trial. Psychother Psychosom. 2012;81(4):217-25. Available from: https://doi.org/10.1159/000335044.
- van Vliet NI, Huntjens RJC, van Dijk MK, Bachrach N, Meewisse ML, de Jongh A. Phase-based treatment versus immediate trauma-focused treatment for post-traumatic stress disorder due to childhood abuse: randomised clinical trial. BJPsych Open. 2021;7(6). Available from: https://doi.org/10.1192/bjo.2021.1057.
- Becker CB, Zayfert C, Anderson E. A survey of psychologists' attitudes towards and utilization of exposure therapy for PTSD. Behav Res Ther. 2004;42(3):277-92. Available from: https://doi.org/10.1016/s0005-7967(03)00138-4.
- van Minnen A, Hendriks L, Olff M. When do trauma experts choose exposure therapy for PTSD patients? A controlled study of therapist and patient factors. Behav Res Ther. 2010;48(4):312-20. Available from: https://doi.org/10.1016/j.brat.2009.12.003.
- Huo Y, Couzner L, Windsor T, Laver K, Dissanayaka NN, Cations M. Barriers and enablers for the implementation of trauma-informed care in healthcare settings: a systematic review. Implement Sci Commun. 2023;4(1):49. Available from: https://doi.org/10.1186/s43058-023-00428-0.
- United Nations Treaty Collection. United Nations convention on the rights of persons with disabilities. New York; 2006. [accessed May 7 2024]. Available from: https://treaties.un.org/Pages/ViewDetails.aspx?src=TREATY&mtdsg_no=iv-15&chapter=4&clang=_en.
- SFS 2017:30. Hälso- och sjukvårdslag. Svensk författningssamling. Stockholm: Socialdepartementet. [accessed 29 Feb 2024]. Available from: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/halso--och-sjukvardslag_sfs-2017-30.
- SFS 2010:Patientsäkerhetslag (2010:659). Svensk författningssamling. [accessed May 7 2024]. Available from: https://www.riksdagen.se/sv/dokument-och-lagar/dokument/svensk-forfattningssamling/patientsakerhetslag-2010659_sfs-2010-659/.
- Lin YK, Liu KT, Chen CW, Lee WC, Lin CJ, Shi L, Tien YC. How to effectively obtain informed consent in trauma patients: a systematic review. BMC Med Ethics. 2019;20(1):8. Available from: https://doi.org/10.1186/s12910-019-0347-0.
- Polismyndigheten. Våldsbrott i nära relationer och sexualbrott mot vuxna: En gemensam granskning av polisens och åklagarens handläggning. Göteborg; 2019. Tillsynsrapport 2019:1. [accessed May 3 2024]. Available from: https://www.aklagare.se/globalassets/dokument/rapporter/tillsynsrapporter/tillsynsrapport-20191-vald-i-nara-relationer-och-sexualbrott-mot-vuxna.pdf.
- Ries NM, Johnston B, Jansen J. A qualitative interview study of Australian physicians on defensive practice and low value care: “It’s easier to talk about our fear of lawyers than to talk about our fear of looking bad in front of each other”. BMC Medical Ethics. 2022;23. Available from: https://doi.org/10.1186/s12910-022-00755-2.
- Pischedda G, Marinò L, Corsi K. Defensive medicine through the lens of the managerial perspective: a literature review. BMC Health Serv Res. 2023;23(1):1104. Available from: https://doi.org/10.1186/s12913-023-10089-3.
- Strobel CJ, Oldenburg D, Steinhäuser J. Factors influencing defensive medicine-based decision-making in primary care: A scoping review. J Eval Clin Pract. 2023;29(3):529-38. Available from: https://doi.org/10.1111/jep.13799.
- Newman E, Kaloupek DG. The risks and benefits of participating in trauma-focused research studies. J Trauma Stress. 2004;17(5):383-94. Available from: https://doi.org/10.1023/B:JOTS.0000048951.02568.3a.
- Galea S, Nandi A, Stuber J, Gold J, Acierno R, Best CL, et al. Participant reactions to survey research in the general population after terrorist attacks. J Trauma Stress. 2005;18(5):461-5. Available from: https://doi.org/10.1002/jts.20053.
- Ferrier-Auerbach AG, Erbes CR, Polusny MA. Does trauma survey research cause more distress than other types of survey research? J Trauma Stress. 2009;22(4):320-3. Available from: https://doi.org/10.1002/jts.20416.
- Campbell R, Adams AE. Why do rape survivors volunteer for face-to-face interviews? A meta-study of victims' reasons for and concerns about research participation. J Interpers Violence. 2009;24(3):395-405. Available from: https://doi.org/10.1177/0886260508317192.
- Brown VM, Strauss JL, LaBar KS, Gold AL, McCarthy G, Morey RA. Acute effects of trauma-focused research procedures on participant safety and distress. Psychiatry Res. 2014;215(1):154-8. Available from: https://doi.org/10.1016/j.psychres.2013.10.038.
- Seedat S, Pienaar WP, Williams D, Stein DJ. Ethics of research on survivors of trauma. Curr Psychiatry Rep. 2004;6(4):262-7. Available from: https://doi.org/10.1007/s11920-004-0075-z.
- Newman E, Risch E, Kassam-Adams N. Ethical issues in trauma-related research: a review. J Empir Res Hum Res Ethics. 2006;1(3):29-46. Available from: https://doi.org/10.1525/jer.2006.1.3.29.
- Keane TM, Najavits LM. Interview: Does Complex Trauma Exist? A “Long View” Based on Science and Service in the Trauma Field. Journal of Clinical Psychology. 2013;69(5):510-5. Available from: https://doi.org/https://doi.org/10.1002/jclp.21991.
- Miller MW, Wolf EJ, Keane TM. Posttraumatic Stress Disorder in DSM-5: New Criteria and Controversies. Clinical Psychology: Science and Practice. 2014;21(3):208-20. Available from: https://doi.org/https://doi.org/10.1111/cpsp.12070.
- Banz L, Stefanovic M, von Boeselager M, Schäfer I, Lotzin A, Kleim B, Ehring T. Effects of current treatments for trauma survivors with posttraumatic stress disorder on reducing a negative self-concept: a systematic review and meta-analysis. Eur J Psychotraumatol. 2022;13(2):2122528. Available from: https://doi.org/10.1080/20008066.2022.2122528.
- White WF, Burgess A, Dalgleish T, Halligan S, Hiller R, Oxley A, et al. Prevalence of the dissociative subtype of post-traumatic stress disorder: a systematic review and meta-analysis. Psychological Medicine. 2022;52(9):1629-44. Available from: https://doi.org/10.1017/S0033291722001647.
- Bækkelund H, Endsjø M, Peters N, Babaii A, Egeland K. Implementation of evidence-based treatment for PTSD in Norway: clinical outcomes and impact of probable complex PTSD. Eur J Psychotraumatol. 2022;13(2):2116827. Available from: https://doi.org/10.1080/20008066.2022.2116827.
- Sele P, Hoffart A, Cloitre M, Hembree E, Øktedalen T. Comparing phase-based treatment, prolonged exposure, and skills-training for Complex Posttraumatic Stress Disorder: A randomized controlled trial. J Anxiety Disord. 2023;100:102786. Available from: https://doi.org/10.1016/j.janxdis.2023.102786.